
Although creatine offers an array of benefits, most people think of it simply as a supplement that bodybuilders and other athletes use to gain strength and muscle mass.
Nothing could be further from the truth. People who don't follow the research on creatine are often stunned to find out how much research has been done, and how many health, fitness, and longevity uses creatine may have.
Why the mainstream media has ignored this fact - in favor of outlandish poorly substantiated scare stories - is unclear, but there has always been a double standard in the mainstream media when it comes to nutritional supplements.
This report will cover much of what creatine has to offer as a safe and inexpensive supplement with an exceptionally wide range of potential uses. Though I will go into depth about each, creatine may positively effect:
- Sarcopenia (a loss of muscle mass due to aging)
- Improve in brain function of healthy and damaged brains
- Modulate inflammation.
- Diseases effecting the neuro muscular system, such as muscular dystrophy (MD)
- Wasting syndromes/muscle atrophy
- Fatigue
- Gyrate atrophy
- Parkinson's disease
- Huntington's disease and other mitochondrial cytopathies
- Neuropathic disorders
- Various dystrophies
- Myopathies
- Various brain pathologies.
- May increasing growth hormone (GH) levels, to those seen with exercise
- Reduce homocysteine levels
- Possibly improving the symptoms of Chronic fatigue Syndrome
- Improve cardiac function in those with congestive heart failure
Creatine is proving to be one of the most promising, well researched, and safe supplements ever discovered for an exceptionally wide range of uses.

Section One
- Creatine is formed in the human body from the amino acids methionine, glycine and arginine. The average person's body contains approximately 120 grams of creatine stored as creatine phosphate.
Certain foods such as beef, herring and salmon, are fairly high in creatine. However, a person would have to eat pounds of these foods daily to equal what can be obtained in one teaspoon of powdered creatine.
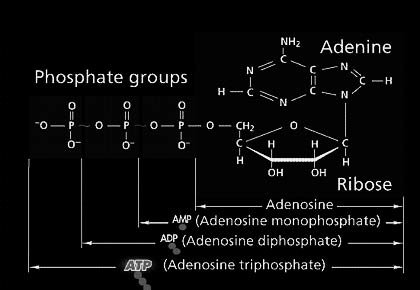
Creatine is directly related to adenosine triphosphate (ATP). ATP is formed in the powerhouses of the cell, the mitochondria. ATP is often referred to as the "universal energy molecule" used by every cell in our bodies.
An increase in oxidative stress coupled with a cell's inability to produce essential energy molecules such as ATP, is a hallmark of the aging cell and is found in many disease states.
Key factors in maintaining health are the ability to:
- Prevent mitochondrial damage to DNA caused by reactive oxygen species (ROS)
- Prevent the decline in ATP synthesis, which reduces whole body ATP levels.
It would appear that maintaining antioxidant status (in particular intra-cellular glutathione) and ATP levels are essential in fighting the aging process.
It is interesting to note that many of the most promising anti-aging nutrients such as CoQ10, NAD, acetyl-l-carnitine and lipoic acid are all taken to maintain the ability of the mitochondria to produce high energy compounds such as ATP and reduce oxidative stress.
The ability of a cell to do work is directly related to its ATP status and the health of the mitochondria. Heart tissue, neurons in the brain and other highly active tissues are very sensitive to this system.
Even small changes in ATP can have profound effects on the tissues' ability to function properly. Of all the nutritional supplements available to us currently, creatine appears to be the most effective for maintaining or raising ATP levels.
- In a nutshell, creatine works to help generate energy. When ATP loses a phosphate molecule and becomes adenosine diphosphate (ADP), it must be converted back to ATP to produce energy. Creatine is stored in the human body as creatine phosphate (CP) also called phosphocreatine.
When ATP is depleted, it can be recharged by CP. That is, CP donates a phosphate molecule to the ADP, making it ATP again. An increased pool of CP means faster and greater recharging of ATP, which means more work can be performed. This is why creatine has been so successful for athletes. For short-duration explosive sports, such as sprinting, weight lifting and other anaerobic endeavors, ATP is the energy system used.
To date, research has shown that ingesting creatine can increase the total body pool of CP which leads to greater generation of energy for anaerobic forms of exercise, such as weight training and sprinting. Other effects of creatine may be increases in protein synthesis and increased cell hydration.
Creatine has had spotty results in affecting performance in endurance sports such as swimming, rowing and long distance running, with some studies showing no positive effects on performance in endurance athletes. Whether or not the failure of creatine to improve performance in endurance athletes was due to the nature of the sport or the design of the studies is still being debated.
Creatine can be found in the form of:
- Creatine monohydrate
- Creatine citrate
- Creatine phosphate
- Creatine-magnesium chelate
- Even liquid versions
However, the vast majority of research to date showing creatine to have positive effects on pathologies, muscle mass and performance used the monohydrate form. Creatine monohydrate is over 90% absorbable, contrary to what some companies and "gurus" have claimed. What follows is a review of some of the more interesting and promising research studies with creatine.
Section Two
So What Can Creatine Potentially Do For Me?"

The Scourge Of Aging:
Sarcopnia & The Potential Role Of Creatine.
- Creatine has been shown to increase strength and muscle mass in young adults in literally dozens of studies at this point. However, there was scant data examining its effects on older adults until more recently. One of the greatest threats to an aging adult's ability to stay healthy and functional is the steady loss of lean bodymass (muscle and bone in particular) as they age.
The medical term for the loss of muscle is sarcopenia, and it's starting to get the recognition it deserves by the medical and scientific community. For decades, that community has focused on the loss of bone mass (osteoporosis) of aging adults but paid little attention to the loss of muscle mass which effects a person's ability to be functional as they age just as much - if not more so - then a loss of bone mass.
What defines sarcopenia from a clinical perspective? Sarcopenia can be defined as the age-related loss of muscle mass, strength and functionality. One thing is very clear: it's far easier, cheaper, and more effective to prevent sarcopenia, or at least greatly slow its progression, then it is to treat it later in life. Sarcopenia generally appears after age of 40 and accelerates after the age of approximately 75.
Although sarcopenia is mostly seen in physically inactive individuals, it is also commonly found in individuals who remain physically active throughout their lives. Thus, it's clear that although physical activity is essential, physical inactivity is not the only contributing factor to sarcopenia.
Just as with osteoporosis, sarcopenia is a multifactorial process that may include decreased hormone levels (in particular, GH, IGF-1, and testosterone), a lack of adequate protein and calories in the diet, oxidative stress, inflammatory processes, as well as a loss of motor nerve cells.
Effects Of Creatine On Older Adults:
- With aging and inactivity, most atrophy an aging person's muscle mass is seen in the fast twitch (FT) fibers which are recruited during high-intensity, anaerobic movements (e.g., weight lifting, sprinting, etc.). Interestingly, these are exactly the fibers creatine has the most profound effects on.
| RELATED ARTICLE | ||
|

- One study called
"Creatine supplementation enhances isometric strength and body composition improvements following strength exercise training in older adults"
- (J Gerontol A Biol Sci Med Sci. 2003 Jan;58(1):11-9.) fed twenty-eight healthy men and women (above 65 years old) either 5 grams per day of creatine or placebo using a random, double-blind protocol for 14 weeks. Both groups were put on a resistance training (weight training) regimen for the duration of the study.
Fourteen weeks of resistance exercise training resulted in significant increases in all measurements of strength and functional tasks and muscle fiber area for both groups.
However, the group getting the creatine resulted in significantly greater increases in fat-free mass, greater increase in isometric knee extension, greater gains in isometric dorsiflexion strength, as well as a significant increase in intramuscular creatine levels. The researchers concluded:
A whole slew of recent studies have been finding similar effects on older adults and coming to virtually identical conclusions. Another recent study entitled "Creatine supplementation improves muscular performance in older men" (Med Sci Sports Exerc. 2002 Mar;34(3):537-43.) using a similar protocol as the aforementioned study found essentially the same effects. They concluded,
"Creatine supplementation may be a useful therapeutic strategy for older adults to attenuate loss in muscle strength and performance of functional living tasks."
Yet more studies (Creatine supplementation combined with resistance training in older men. Med Sci Sports Exerc. 2001 Dec;33(12):2111-7.) has come to similar conclusions. However, it should be noted that not all studies have found this effect (Effects of creatine monohydrate ingestion in sedentary and weight-trained older adults. Acta Physiol Scand. 1998 Oct;164(2):147-55.) but they were earlier studies that may have had some methodological flaws.
Regardless, the bulk of the data, in particular the recent data, clearly points to creatine as having positive effects on strength and body composition in older adults, especially when combined with a resistance training exercise protocol.
One particularly interesting recent study found the positive effects of creatine on strength and lean tissue in older adults continued after they stopped using the creatine (Effect of Ceasing Creatine Supplementation While Maintaining Resistance Training in Older Men. JAPA, 12(3), July 2004,), at least for the 12 weeks they tested them. They concluded,
However, it's the experience of most creatine users, as well as most studies in younger adults, that the positive effects of creatine do in fact fade over time if one stops using creatine. Thus, being there is no particular reason to go off creatine once started, best effects will probably come from continues use.
The Real Secret To Aging:
Cellular Energetics.
- What's really the major difference between an older adult and a younger adult? Cellular energetics is the answer: the ability of each cell in our body to regulate its ability to produce energy (e.g., ATP), detoxify harmful compounds, and defend itself against free radical damage and other assaults.
An increase in oxidative stress coupled with a cell's inability to produce essential energy molecules such as ATP, is a hallmark of the aging cell and is found in many disease states.
A younger persons' cells are quite efficient at dealing with those problems faced by the cell, an older person's cells, be it brain cells, muscle cells, etc. are unable to deal with these challenges, and over time damage accumulates, and the cell dies.
In younger healthy adults, old cells are replaced by new healthy cells rapidly, but that's not the case the older we get.
The decline in muscle mass (sarcopenia) with aging may be related to a decline in mitochondrial function. Without these high energy compounds, which every cell in our body depends to function, the cell and the entire organism (us!) dies.
| RECOMMENDED LINK | ||
|

- It's been established that older adults tend to have lower tissue levels of creatine phosphate (CP), ATP, and other essential high energy molecules. Older individuals appear to respond differently to exercise also in terms of replenishing these essential molecules after exercise.
One study called "Skeletal muscle mitochondrial function and lean body mass in healthy exercising elderly" (Mech Ageing Dev. 2003 Mar;124(3):301-9.) measured mitochondrial function and recovery time in , 45 older (average age 73), and 20 younger subjects (average age 25) who were matched for body mass.
They then had the two groups exercise at different intensity levels. As other studies have found, older people in the group had lower baseline CP and ATP levels then their younger counterparts and they were slower to replenish tissue levels after exercise. As the researchers put it,
Translated, not only did the older subjects have lower levels of essential high energy compounds (e.g. ATP, CP, etc.) to begin with compared to the younger group, it was made worse the more intense the exercise! As the studies above with older adults show, creatine in supplemented form can ameliorate some of that decline.
Creatine may be one of the most effective and safe non-prescription compounds currently available to improve cellular energetics (the ability of the cells to produce energy which keeps us alive!) and may be an effective treatment for sarcopenia, especially when combined with the proper exercise regimen.
To sum up this section, the two essential strategies to help prevent the decline in cellular health, which appears linked to sarcopenia and other issues faced by an aging person:
- prevent concomitant decline in ATP/CP levels which reduces whole body ATP levels that leads to sarcopenia and many other pathologies, via creatine supplements and others that maintain cellular energetics (e.g., acetyl L-carnitine, alpha lipoic acid, QoQ10. etc.)
- Increase or maintain intra cellular glutathione and improve mitochondrial anti oxidant status (to prevent mitochondrial damage to DNA caused by reactive oxygen species) by taking anti oxidants and or nutrients known to improve anti oxidant status (e.g. whey protein, NAC, etc).
It would appear that maintaining mitochondrial anti oxidant status (in particular intra cellular glutathione) and ATP levels, is an essential combination in fighting the aging process as well as combating/preventing a host of diseases.
Anti-Inflammatory Effects Of Creatine:
- Interestingly, though not surprisingly, creatine may have the ability to modulate inflammation, at least after exercise. One study entitled "The effect of creatine supplementation upon inflammatory and muscle soreness markers after a 30km race" (
Life Sci.
- 2004 Sep 3;75(16):1917-24.) examined this issue. The researchers looked at the effect of creatine on inflammatory and muscle soreness markers:
- Creatine kinase (CK)
- Lactate dehydrogenase (LDH)
- Prostaglandin E2 (PGE2)
- Tumor necrosis factor-alpha (TNF-alpha)
in experienced runners after running 30km.
Runners were supplemented for 5 days prior to the 30km race with 4 doses of 5g of creatine and 15g of maltodextrine per day while the control group received the same amount of maltodextrine. Pre-race blood samples were collected before running the 30km, immediately after the race, and 24 hours after the end of the run.
As one would expect, the control group had large increases in CK, LDH, PGE2, and TNF-alpha concentrations. In fact, there was over a four fold increase in CK, 43% increase in LDH, over a 6 fold increase in PGE2, and a doubling of TNF-alpha!
This indicates a high level of cell injury and inflammation in these athletes. However, the group getting the creatine had far lower indicators of cellular damage and inflammation, with a 19% increase in CK, 70% increase in PGE2, and a 34% increase in TNF-alpha. Creatine supplementation totally abolished the increase in LDH. No side effects at all were reported by the athletes getting the creatine. The researchers concluded,
There are a few comments and questions to be made regarding these findings. Regular exercise is an essential component for any person looking to improve their health, keep bodyfat low, retain essential muscle mass as they age, etc., but it also has it's downsides, such as increased free radical production and other effects the body has to combat.
Creatine may be a key nutrient here. However, it's unclear if it works in more moderate physical endeavors (as not everyone is running 30km races all the time!) and whether it would have the same effects on inflammatory markers in non-exercising people. None the less, the results are compelling and add to the long list the potential benafits of creatine.
Creatine Effects On The Function
Of Healthy & Damaged Brains:
- Perhaps the most compelling use for creatine is its effects on brain function and metabolism. I covered some of those effects in the past two articles but research continues to show creatine is a key nutrient for brain function and metabolism in both people with healthy or damaged/diseased brains.
Traumatic brain injuries affect thousands of people each year. The real tragedy however is that much of the damage to the brain is not caused by the immediate injury, but due to cell death caused by ischemia (a lack of blood flow and oxygen to tissues) and free radical damage/oxidative stress.
The ability of a cell to do work is directly related to its ATP status and the health of the mitochondria. Heart tissue, neurons in the brain and other highly active tissues are very sensitive to this system.
Even small changes in ATP can have profound effects on the tissues' ability to function properly, which can cause damage and or death for the cell. Of all the nutritional supplements available to us currently, creatine appears to be the most effective for maintaining or raising ATP levels.
Recent studies have shown that creatine affords significant neuroprotection against ischemic and oxidative insults. One recent study called "Dietary supplement creatine protects against traumatic brain injury" (Ann Neurol. 2000 Nov;48(5):723-9.) found creatine was very effective at reducing damage to brain tissue after injury. These researchers found,
They went on to conclude:
This study would indicate creatine therapy should be initiated as soon as possible after traumatic brain injury. People who have already been taking creatine on a continuous basis may be afforded considerable protection against additional damage to the brain following such an injury.
- But what about the healthy brain you ask? No, you don't need to injure your brain in an auto accident to get benafits! A recent study entitled
"Oral creatine monohydrate supplementation improves brain performance: a double-blind, placebo controlled, cross-over trial"
- (Proceedings of the Royal Society: Biological Sciences Vol. 270, No. 1529 on 22 October 2003.) found that six weeks of creatine supplementation at 5g per day to 45 five vegetarians using a double blind placebo cross over designed study, greatly improved cognitive function. According the report put out by The Royal Society,
Though creatine supplementation would probably have a less dramatic effect on non-vegetarians -due to the fact they get some creatine in their diet from the meat they eat - it stands to reason creatine will still be effective for improving creatine levels in the brain of meat eaters and vegetarians alike. Healthy and injured brains alike appear to benefit from creatine!
Creatine & Neuromuscular Diseases:
- One of the most promising areas of research with creatine is its effect on neuromuscular diseases such as MD. One study looked at the safety and efficacy of creatine monohydrate in various types of muscular dystrophies using a double blind, crossover trial.
Thirty-six patients (12 patients with facioscapulohumeral dystrophy, 10 patients with Becker dystrophy, eight patients with Duchenne dystrophy and six patients with sarcoglycan-deficient limb girdle muscular dystrophy) were randomized to receive creatine or placebo for eight weeks.
The researchers found there was a "mild but significant improvement" in muscle strength in all groups. The study also found a general improvement in the patients' daily-life activities as demonstrated by improved scores in the Medical Research Council scales and the Neuromuscular Symptom scale. Creatine was well tolerated throughout the study period, according to the researchers.1
Another group of researchers fed creatine monohydrate to people with neuromuscular disease at 10 grams per day for five days, then reduced the dose to 5 grams per day for five days.
The first study used 81 people and was followed by a single-blinded study of 21 people. In both studies, body weight, handgrip, dorsiflexion and knee extensor strength were measured before and after treatment. The researchers found,
Short-term creatine monohydrate increased high-intensity strength significantly in patients with neuromuscular disease.2 There have also been many clinical observations by physicians that creatine improves the strength, functionality and symptomology of people with various diseases of the neuromuscular system.
More Brain Related Research:
Creatine & Neurological Protection.
- If there is one place creatine really shines, it's in protecting the brain from various forms of neurological injury and stress. A growing number of studies have found that creatine can protect the brain from neurotoxic agents, certain forms of injury and other insults.
Several in vitro studies found that neurons exposed to either glutamate or beta-amyloid (both highly toxic to neurons and involved in various neurological diseases) were protected when exposed to creatine.3 The researchers hypothesized that,
More recent studies, in vitro and in vivo in animals, have found creatine to be highly neuroprotective against other neurotoxic agents such as N-methyl-D-aspartate (NMDA) and malonate.4
Another study found that feeding rats creatine helped protect them against tetrahydropyridine (MPTP), which produces parkinsonism in animals through impaired energy production. The results were impressive enough for these researchers to conclude,
Other studies have found creatine protected neurons from ischemic (low oxygen) damage as is often seen after strokes or injuries.6
Yet more studies have found creatine may play a therapeutic and or protective role in Huntington's disease7, 8 as well as ALS (amyotrophic lateral sclerosis).9 This study found that
Amazingly, this is only the tip of the iceberg showing creatine may have therapeutic uses for a wide range of neurological disease as well as injuries to the brain.
- Because it is known that heart cells are dependent on adequate levels of ATP to function properly, and that cardiac creatine levels are depressed in chronic heart failure, researchers have looked at supplemental creatine to improve heart function and overall symptomology in certain forms of heart disease.
It is well known that people suffering from chronic heart failure have limited endurance, strength and tire easily, which greatly limits their ability to function in everyday life.
Using a double blind, placebo-controlled design, 17 patients aged 43 to 70 years with an ejection fraction <40 were supplemented with 20 grams of creatine daily for 10 days. Before and after creatine supplementation, the researchers looked at:
- Ejection fraction of the heart (blood present in the ventricle at the end of diastole and expelled during the contraction of the heart)
- 1-legged knee extensor (which tests strength)
- Exercise performance on the cycle ergometer (which tests endurance)
Biopsies were also taken from muscle to determine if there was an increase in energy-producing compounds (i.e., creatine and creatine phosphate). Interestingly, but not surprisingly, the ejection fraction at rest and during the exercise phase did not increase.
However, the biopsies revealed a considerable increase in tissue levels of creatine and creatine phosphate in the patients getting the supplemental creatine.
More importantly, patients getting the creatine had increases in strength and peak torque (21%, P < 0.05) and endurance (10%, P < 0.05). Both peak torque and 1-legged performance increased linearly with increased skeletal muscle phosphocreatine (P < 0.05). After just one week of creatine supplementation, the researchers concluded:
Another study looked at the effects of creatine supplementation on endurance and muscle metabolism in people with congestive heart failure.11
In particular the researchers looked at levels of ammonia and lactate, two important indicators of muscle performance under stress. Lactate and ammonia levels rise as intensity increases during exercise and higher levels are associated with fatigue.
High-level athletes have lower levels of lactate and ammonia during a given exercise than non-athletes, as the athletes' metabolism is better at dealing with these metabolites of exertion, allowing them to perform better.
This study found that patients with congestive heart failure given 20 grams of creatine per day had greater strength and endurance (measured as handgrip exercise at 25%, 50% and 75% of maximum voluntary contraction or until exhaustion) and had lower levels of lactate and ammonia than the placebo group.
This shows that creatine supplementation in chronic heart failure augments skeletal muscle endurance and attenuates the abnormal skeletal muscle metabolic response to exercise.
It is important to note that the whole-body lack of essential high energy compounds (e.g. ATP, creatine, creatine phosphate, etc.) in people with chronic congestive heart failure is not a matter of simple malnutrition, but appears to be a metabolic derangement in skeletal muscle and other tissues.12
Supplementing with high energy precursors such as creatine monohydrate appears to be a highly effective, low cost approach to helping these patients live more functional lives, and perhaps extend their life spans.
| RECOMMENDED LINK | ||
|
Download the Full Text!
- Walter MC, et al. Creatine monohydrate in muscular dystrophies: A double blind, placebo-controlled clinical study. Neurology 2000 May 9; 54(9): 1848-50.
- Tarnopolsky M, et al. Creatine monohydrate increases strength in patients with neuromuscular disease. Neurology 1999 Mar 10; 52(4): 854-7.
- Protective effect of the energy precursor creatine against toxicity of glutamate and beta-amyloid in rat hippocampal neurons. J Neurochem 1968-1978; 74(5).
- Malcon C, et al. Neuroprotective effects of creatine administration against NMDA and malonate toxicity. Brain Res 2000; 860(1-2): 195-8.
- Matthews RT, et al. Creatine and cyclocreatine attenuate MPTP neurotoxicity. Exp Neurol 1999; 157(1): 142-9.
- Balestrino M, et al. Role of creatine and phosphocreatine in neuronal protection from anoxic and ischemic damage. Amino Acids Abstract 2002; 23(1-3): 221-229.
- Matthews RT, et al. Neuroprotective effects of creatine and cyclocreatine in animal models of Huntington's disease. J Neurosci 1998; 18(1): 156-163.
- Ferrante RJ, et al. Neuroprotective effects of creatine in a transgenic mouse model of Huntington's disease. J Neurosci 2000; 20(12): 4389-97.
- Klivenyi P, et al. Neuroprotective effects of creatine in a transgenic animal model of amyotrophic lateral sclerosis. Nat Med 1999; 5(3): 347-50.
- Gordon A, et al. Creatine supplementation in chronic heart failure increases skeletal muscle creatine phosphate and muscle performance. Cardiovasc Res 1995 Sep; 30(3): 413-8.
- Andrews R, et al. The effect of dietary creatine supplementation on skeletal muscle metabolism in congestive heart failure. Eur Heart J 1998 Apr; 19(4): 617-22.
- Broqvist M, et al. Nutritional assessment and muscle energy metabolism in severe chronic congestive heart failure-effects of long-term dietary supplementation. Eur Heart J 1994 Dec; 15(12): 1641-50.
- Park JH, et al. Use of P-31 magnetic resonance spectroscopy to detect metabolic abnormalities in muscles of patients with fibromyalgia. Arthritis Rheum 1998 Mar; 41(3): 406-13.